Important Questions for First Sessional Examination.
-
Long Questions:
-
Explain the significance of controlled release systems and their design. Explain the physiological and biochemical features of Controlled Drug Delivery Systems.
Answer::
-
Definition: Controlled drug delivery is one which delivers the drug at a predetermined rate, locally or systemically, for a specified period of time.
-
However it is observed that many terms are used synonymously, to differentiate them from one another we are going to discuss different terminologies that are used in NDDS related to controlled release formulations.
-
Rationale:
-
To provide a location-specific action within the GIT.
-
To avoid an undesirable local action within the GIT.
-
To provide a programmed drug delivery pattern.
-
To increase the rate and extent of absorption/bioavailability.
-
To extend the duration of action of the drug.
-
Significance:
-
Maintains the drug level within the desired range.
-
Useful for delivery of "difficult"’ drugs: the slow release of water-soluble drugs, and/or fast release of poorly soluble drugs,
-
Reduces dosing frequency,
-
Avoids over or underdosing,
-
Prevention or reduction of side effects,
-
Reduction in total health care cost,
-
Improved efficacy in the treatment,
-
Reduction in adverse side effects and improvement in tolerability
-
Improved patient compliance,
-
Uses less amount of total drug,
-
Minimizes or removes local or systemic side effects.
-
Minimal drug accumulation on chronic usage
-
Cures or controls the condition more promptly
-
Reduces the fluctuation in drug level
-
Improves the bioavailability of some drugs.
-
Approaches to design formulations:
-
Based on the mechanism of drug-release and carrier used, the modified-release dosage form can be classified into the following six categories;
-
Diffusion based system.
-
Reservoir type.
-
Matrix type.
-
Dissolution based system.
-
Reservoir type.
-
Matrix type.
-
Methods using Ion-exchange.
-
Methods using osmotic pressure.
-
pH-independent formulations.
-
Altered-density formulations.
-
Physiological and biochemical features of Controlled Drug Delivery Systems.
-
Biopharmaceutical characteristics of the drug:
-
The molecular weight of the drug
-
The aqueous solubility of the drug
-
Apparent partition coefficient
-
Drug pKa and ionization physiological pH
-
Drug stability
-
Mechanism and site of absorption
-
Route of administration.
-
Pharmacokinetic characteristics of the drug:
-
Absorption rate
-
Elimination half-life
-
Rate of Metabolism
-
Absolute bioavailability
-
Total clearance (CL)
-
Apparent volume of distribution (VD)
-
Therapeutic concentration (Css)
-
Pharmacodynamic characteristic of the drug:
-
Therapeutic index
1.1 The molecular weight of the drug:
-
Small molecules may pass through pores of a membrane by convective transport.
-
This applies to both, the drug release from the dosage form and the transport across a biological membrane.
-
For biologic membranes the limit may be a molecular weight of 150 and 400 respectively for spherical molecules and chain-like compounds respectively.
1.2 Solubility:
-
For all mechanisms of absorption the drug must be present at the site of absorption in the form of solution.
-
During the Preformulation study it is necessary to determine the solubility of the drug at various pH values.
-
If the solubility is less than 0.1 μg/ml (in acidic medium) one may expect reduced bioavailability.
-
It seems that drugs are well absorbed by passive diffusion from the small intestine upon oralApparent partition coefficient (APC) administration if at least 0.1 to 1% is non ionized form.
1.3 Apparent partition coefficient (APC):
-
Drugs being absorbed by passive diffusion must have a certain minimal APC.
-
The higher the APC in an n-octanol/buffer system the higher is the flux across a membrane for many drugs.
-
The APC should be determined for the entire pH range in the GI tract.
-
The APC must also be applied for partition of the drug between CRDDS and the biological fluid.
1.4 General absorption mechanism:
-
For a drug to be a variable candidate for per oral CRDDS, its absorption mechanism must be by diffusion throughout the entire GI tract.
-
The term diffusion here refers to the dual pathway of absorption either by partitioning into the lipid membrane (across the cells) or by passing through water filled channels (between the cells).
-
It is also important that absorption occurs from all segments of the GI tract which may depend on the drug’s pKa, the pH in the segment, binding of drug to mucus, blood flow rate, etc.
-
In any case, the drug release from the CRDDS should not be influenced by pH changes within the GI tract, by enzymes present in the lumen, peristalsis, etc.
-
The one compartment open model is quite suitable to design CRDDS for most drugs.
2.1 Absorption Rate:
-
In order to ensure that the release process is the rate controlling step, the intrinsic absorption rate constant should be higher than the desired release rate constant of the drug from the dosage form.
2.2 Elimination half-life:
-
Drugs having a t ½ of 8 hours are ideally suited for CRDDS.
-
If the t ½ is less than 1 hour the dose size required for a 12 hour or 24 hour duration dosage form may be too large.
-
If the t ½ is very long there is usually no need for a CRDDS.
2.3 Rate of metabolism:
-
The rate of metabolism directly affects the t ½ of the drug.
-
There are two areas of concern related to metabolism that significantly restrict CRDDS product design.
-
First, if a drug, upon chronic administration, is capable of either inducing or inhibiting enzyme synthesis, it will be a poor candidate for a S/R/C.R product because of the difficulty of maintaining uniform blood levels of a drug.
-
Second, if there is a variable blood level of a drug through either intestinal (or tissue) metabolism or through first pass effect.
2.4 Absolute Bioavailability:
-
The absolute bioavailability is the percentage of drug taken up into systemic circulation upon extravascular administration.
-
For drugs to be suitable for CRDDS this value should be close to 100%.
2.5 Total clearance (CL):
-
CL is a measure of the volume of distribution cleared of drugs per unit of time.
-
It is the key parameter in estimating the required dose rate for CRDDS, and predicting the steady state concentration.
2.6 Apparent volume of distribution (VD):
-
The Volume of distribution (VD), also known as the apparent volume of distribution, is used to quantify the distribution of a drug between plasma and the rest of the body after oral or parenteral dosing.
-
It is defined as the volume in which the amount of drug would be uniformly distributed to produce the observed blood concentration.
-
The apparent volume of distribution is a proportionality constant relating the plasma concentration to the total amount of drug in the body.
2.7 Therapeutic concentration (Css):
-
The therapeutic concentrations are the desired or target steady state peak concentrations (Css max), the desired or target steady state minimum concentrations (Css min), and the mean steady state concentration (Css avg).
-
The difference between Css max and Css min is the fluctuation.
-
The smaller the desired fluctuation the greater must be the precision of the dosage form performance.
-
The lower Css, the smaller Vz, the longer t ½, the higher F and The less amount of drug is
-
required to be incorporated into a CRDDS.
3.1 Therapeutic index:
-
It is most commonly used to calculate a drug's safety margin.
-
TI = TD 50 /ED50
-
The longer the value of TI, the safer the drug.
-
Drugs with very small value of Therapeutic index are poor candidates for formulation into CRDDS products.
-
A drug is considered to be safe if its T.I value is greater than 10.
b) What are polymers? Discuss the advantages and classification of polymers.
Answer:
-
Definition: “Polymer” is derived from Greek words “Poly'' meaning many and “Meros” meaning parts.
-
Polymers have very large molecular weights and are made up of repeating units (or monomers) throughout their chains.
-
Advantages:
-
Selective Targeting: Polymers can facilitate selective targeting, allowing drugs to be delivered specifically to the desired site within the body.
-
2. Enhanced Circulation: Polymers can prolong drug circulation in the bloodstream, ensuring sustained therapeutic effects.
-
3. Improved Delivery: Polymers enable controlled release of drug cargo, maintaining optimal drug levels over time.
-
4. Biodegradability: Biodegradable polymers break down naturally in the body, minimising long-term impact and reducing toxicity.
-
5. Bioavailability: Polymers enhance drug bioavailability by improving solubility and absorption.
-
6. Non-Toxicity: Many polymers used in drug delivery systems are non-toxic and biocompatible.
-
7. Flexibility in Composition: Polymer-based systems allow flexibility in design due to their nano-level structure.
-
8. Stability: Polymers protect drugs from degradation, ensuring stability during storage and transport.
-
9. Controlled Release Rates: Incorporating biodegradable polymers in tablet matrices allows precise control over drug release rates.
-
10. Safe Framework: Whether through implants or other delivery methods, biodegradable polymers provide a safe framework for drug delivery without harm to the body.
-
Classification:
Classification of Polymers Based on the Origin
-
Natural Polymers
-
Protein-based:
-
Albumin, collagen, gelatin, etc.
-
Polysaccharides:
-
Agarose, alginate, carrageenan, chitosan, cyclodextrins, dextran, hyaluronic acid, polysialic acid, etc.
-
Synthetic Polymers
-
Biodegradable Polyesters:
-
Poly(lactic acid) (PLA), poly (glycolic acid) (PGA), poly (hydroxybutyrate) (PHB), poly (Ɛ-caprolactone) (PCL), poly(β-malic acid) (PMA), poly(dioxanes) (PDA) etc.
-
Polyanhydrides:
-
Poly(sebacic acid) (PSBA), poly(adipic acid) (PAPA), poly(terephthalic acid) (PTA) and various copolymers etc. Polyamides include poly(imino carbonates) (PIC), polyamino acids (PAA), and others.
-
Phosphorus-based:
-
polyphosphates, polyphosphonates, polyphosphazenes, etc.
-
Others:
-
Poly(cyanoacrylates) (PCA), polyurethanes, polyortho esters, polydihydropyrans,polyacetals etc.
-
Non-biodegradable Cellulose derivatives:
-
carboxymethyl cellulose (CMC), ethylcellulose (EC), cellulose acetate (CA), cellulose acetate propionate (CAP), hydroxypropyl methylcellulose (HPMC), etc.
-
Silicones:
-
Polydimethylsiloxane (PDS), colloidal silica, etc.
-
Acrylic polymers:
-
Polymethacrylates (PMA), poly(methyl methacrylate) (PMMA), poly hydro(ethyl methacrylate) (PHEM) etc.
-
Others:
-
Polyvinyl pyrrolidone (PVP), Ethyl Vinyl Acetate (EVA), poloxamers, poloxamines, etc.
-
Semi-synthetic Polymer:
-
Hydrogenated natural rubber, cellulose nitrate, methyl cellulose, etc. are chemically modified polymers.
Ideal Characters of polymers
-
It should be inert and compatible with the environment.
-
It should be non- toxic and physiologically inert.
-
It should be easily administrable.
-
It should be easy to fabricate and must be inexpensive.
-
It should have good mechanical strength.
-
It must have compatibility with most of the drugs.
-
It must not adversely affect the rate of release of the drug.
-
It must not have tendency to retain in tissue and must be a good biodegradable material.
c) Classify controlled release drug delivery systems. Describe matrix systems.
Discuss advantages of controlled release drug delivery systems.
Answer:
-
Definition: Controlled drug delivery is one which delivers the drug at a predetermined rate, locally or systemically, for a specified period of time.
-
However it is observed that many terms are used synonymously, to differentiate them from one another we are going to discuss different terminologies that are used in NDDS related to controlled release formulations.
-
Classification:
-
Diffusion based system.
-
Reservoir type.
-
Matrix type.
-
Dissolution based system.
-
Reservoir type.
-
Matrix type.
-
Methods using Ion-exchange.
-
Methods using osmotic pressure.
-
pH-independent formulations.
-
Altered-density formulations.
-
Advantages:
-
Maintains the drug level within the desired range.
-
Useful for delivery of "difficult"’ drugs: the slow release of water-soluble drugs, and/or fast release of poorly soluble drugs,
-
Reduces dosing frequency,
-
Avoids over or underdosing,
-
Prevention or reduction of side effects,
-
Reduction in total health care cost,
-
Improved efficacy in the treatment,
-
Reduction in adverse side effects and improvement in tolerability
-
Improved patient compliance,
-
Uses less amount of total drug,
-
Minimises or removes local or systemic side effects.
-
Minimal drug accumulation on chronic usage
-
Cures or controls the condition more promptly
-
Reduces the fluctuation in drug level
-
Improves the bioavailability of some drugs.
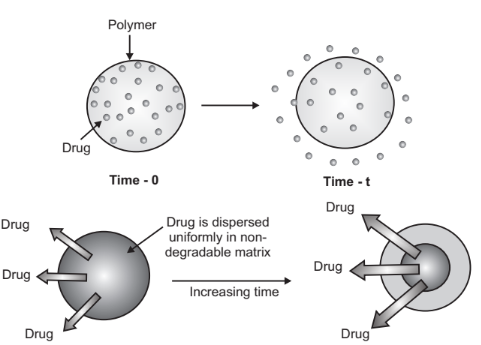
Matrix System:
-
Drugs are uniformly distributed throughout a polymer matrix in a matrix device.
-
In this model, the drug first dissolves and then diffuses out of the matrix in the outer layer that is exposed to the bathing solution.
-
The interaction between the bathing solution and the solid drug moves toward the interior as this process continues.
2. Short Questions:
-
Describe Ion Exchange Resins based controlled release formulation.
Answer:
-
Ion-exchange systems generally use resins composed of water-insoluble, cross-linked polymers.
-
These polymers contain salt-forming functional groups in repeating positions on the polymer chain.
-
The drug is bound to the resin and released by exchanging with appropriately charged ions in contact with the ion-exchange groups.
-
Resin+ − Drug− + X− → resin+ − X− + Drug−
-
Conversely,
-
Resin− − Drug+ + Y+ → Resin− − Y+ + Drug+
-
Where, X− and Y+ are ions in the GI tract.
-
The free drug then diffuses out of the resin.
-
The resin is combined with the drug solution to create the drug-resin complex, either by repeatedly exposing the resin to the drug in a chromatography column or by allowing it to remain in the solution for an extended period of time.
-
The amount of crosslinking agent used to prepare the resin affects the resin's rigidity, diffusional path length, and area of diffusion, all of which affect how quickly drugs diffuse out of it.
-
This system is beneficial for drugs that are highly susceptible to enzymatic degradation because it provides a protective mechanism by temporarily altering the substrate.
-
The limitation of this approach to controlled release is that the release rate is proportional to the concentration of ions present in the area of administration.
-
The release rate of the drug can be impacted by variations in diet, water intake, and individual intestinal content even though the ionic concentration of the GI tract is relatively constant within bounds.
-
An improvement in this system is to coat the ion-exchange resin with a hydrophobic rate-limiting polymer, such as ethyl cellulose or waxes. These systems rely on the polymer coat to govern the rate of drug availability.
-
For this system to be diffusion controlled, it is obvious that the rate of drug particle dissolution within the matrix must be much faster than the rate of drug dissolution leaving the matrix.
-
What are biodegradable and non- biodegradable polymers, give examples of each?
Answer:
Biodegradable polymers: The polymers which are degraded inside the body by various means are called biodegradable polymers.
e.g. Chitosan, Poly(lactic acid) (PLA).
Non-biodegradable polymers: The polymers which are not degraded inside the body by any means are called biodegradable polymers.
e.g. carboxymethyl cellulose (CMC), hydroxypropyl methylcellulose (HPMC).
-
Classify the polymers.
Answer:
Classification of Polymers Based on the Origin
-
Natural Polymers
-
Protein-based:
-
Albumin, collagen, gelatin, etc.
-
Polysaccharides:
-
Agarose, alginate, carrageenan, chitosan, cyclodextrins, dextran, hyaluronic acid, polysialic acid, etc.
-
Synthetic Polymers
-
Biodegradable Polyesters:
-
Poly(lactic acid) (PLA), poly (glycolic acid) (PGA), poly (hydroxybutyrate) (PHB), poly (Ɛ-caprolactone) (PCL), poly(β-malic acid) (PMA), poly(dioxanes) (PDA) etc.
-
Polyanhydrides:
-
Poly(sebacic acid) (PSBA), poly(adipic acid) (PAPA), poly(terephthalic acid) (PTA) and various copolymers etc. Polyamides include poly(imino carbonates) (PIC), polyamino acids (PAA), and others.
-
Phosphorus-based:
-
polyphosphates, polyphosphonates, polyphosphazenes, etc.
-
Others:
-
Poly(cyanoacrylates) (PCA), polyurethanes, polyortho esters, polydihydropyrans,polyacetals etc.
-
Non-biodegradable Cellulose derivatives:
-
carboxymethyl cellulose (CMC), ethylcellulose (EC), cellulose acetate (CA), cellulose acetate propionate (CAP), hydroxypropyl methylcellulose (HPMC), etc.
-
Silicones:
-
Polydimethylsiloxane (PDS), colloidal silica, etc.
-
Acrylic polymers:
-
Polymethacrylates (PMA), poly(methyl methacrylate) (PMMA), poly hydro(ethyl methacrylate) (PHEM) etc.
-
Others:
-
Polyvinyl pyrrolidone (PVP), Ethyl Vinyl Acetate (EVA), poloxamers, poloxamines, etc.
-
Semi-synthetic Polymer:
-
Hydrogenated natural rubber, cellulose nitrate, methyl cellulose, etc. are chemically modified polymers.
Based on the types of monomer:
-
Homopolymer:
-
A polymer containing a single type of repeat units is called a homopolymer.
-
e.g., polystyrene.
-
Copolymer:
-
If a polymer is made up of two different monomers then it is called copolymer.
-
e.g., styrene butadiene (SBS) rubber and Sty-co-An.
D. Write about reservoir and matrix type of controlled release formulations.
Answer:
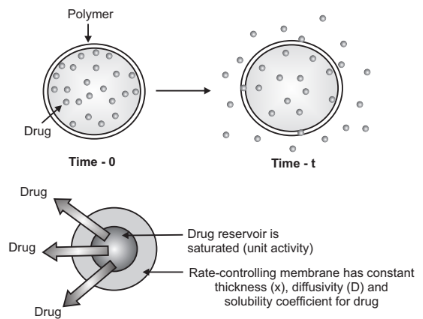
Reservoir Devices:
-
Reservoir devices are characterized by a core of the drug, the reservoir, surrounded by a polymeric membrane.
-
The nature of the membrane determines the rate of release of drugs from the system.
-
The advantages of reservoir diffusional systems are, zero-order delivery is possible and the release rate will vary with polymer type.
-
The disadvantages of reservoir diffusional systems are, a system must be physically planted, it is difficult to deliver high-molecular-weight compounds, and rupture can result in dangerous dose dumping.
Matrix Devices:
-
Drugs are uniformly distributed throughout a polymer matrix in a matrix device.
-
In this model, the drug first dissolves and then diffuses out of the matrix in the outer layer that is exposed to the bathing solution.
-
The interaction between the bathing solution and the solid drug moves toward the interior as this process continues.
-
For this system to be diffusion controlled, it is obvious that the rate of drug particle dissolution within the matrix must be much faster than the rate of drug dissolution leaving the matrix.
e. Enlist and define various terminologies used in CDDS.
Answer: Different terms used in novel drug delivery systems,
-
Delayed-Release:
-
A dosage form that releases a separate fraction of the drug at a time or times other than administration, although one portion may be released immediately after administration.
-
e.g. ; enteric-coated tablets, where a timed-release is achieved by barrier coating repeated action tablets or spansules.
-
Extended-Release:
-
When absorption of the drug is greater than its elimination, the release is known as extended-release.
-
A dosage form should allow at least a two fold reduction in dosage frequency as compared to that drug presented as an immediate release dosage form.
-
These include; any dosage form that maintains the therapeutic blood or tissue level of the drug for a prolonged period of time.
-
Sustained Release:
-
It includes the drug delivery systems that achieve and ensure a slow release of drugs over an extended/prolonged period or at a constant release rate to attain and maintain therapeutically effective levels of drug concentration in the circulation.
-
Here the absorption rate is equal to the elimination rate over an extended period.
-
Controlled Release:
-
It includes any drug delivery system by which the drug is delivered at a predetermined rate over a prolonged period.
-
Site-Specific Targeting:
-
It is a dosage form that releases drugs at or near the intended physiologic site of action.
-
Targeted release dosage forms may have either immediate or extended-release characteristics.
-
They usually contain suitable site directing molecules, which recognize their receptor or molecular attachment sites at the target.
-
Receptor Targeting:
-
In this type of system, the target is a particular receptor within an organ or tissue.
-
Fast Dissolve Drug Delivery System:
-
Also called Flash release systems.
-
It is a type of solid dosage form that dissolves or disintegrates in the oral cavity without the help of water or chewing.
-
Fast dissolution is achieved by forming,
-
a loose network, or by effervescent agent, or with a mixture of disintegrating agents.
3. Short Questions:
-
What are ideal characters of polymers?
Answer: Ideal Characters of polymers
- It should be inert and compatible with the environment.
-
It should be non- toxic and physiologically inert.
-
It should be easily administrable.
-
It should be easy to fabricate and must be inexpensive.
-
It should have good mechanical strength.
-
It must have compatibility with most of the drugs.
-
It must not adversely affect the rate of release of the drug.
-
It must not have tendency to retain in tissue and must be a good biodegradable material.
b. Define Passive Diffusion and Active Transport.
Answer:
Passive Diffusion
Passive diffusion is the movement of molecules or ions from an area of higher concentration to an area of lower concentration, without the need for energy input. This process relies on the natural kinetic energy of the molecules and the entropy of the system. Examples of passive diffusion include the movement of oxygen and carbon dioxide across cell membranes.
Active Transport
Active transport is the movement of molecules or ions against their concentration gradient, from an area of lower concentration to an area of higher concentration. This process requires energy, usually in the form of ATP, and involves specific transport proteins embedded in the cell membrane. Examples of active transport include the sodium-potassium pump and the uptake of glucose in the intestines.
c. What are the stages in mucoadhesion?
Answer:
Mucoadhesion involves the process by which a drug delivery system adheres to the mucosal tissues. This process can be broken down into several stages:
-
Wetting and Swelling: The initial stage involves the wetting and swelling of the polymer. This allows the polymer to come into close contact with the mucosal surface.
-
Interpenetration: In this stage, the polymer chains interpenetrate with the mucin chains present in the mucus layer. This interpenetration is crucial for forming a strong adhesive bond.
-
Formation of Chemical Bonds: Finally, chemical bonds such as hydrogen bonds, ionic bonds, and van der Waals forces form between the polymer and the mucosal surface, consolidating the adhesive interaction.
These stages ensure that the drug delivery system remains in close contact with the mucosal surface, enhancing drug absorption and efficacy.
D. Why drugs having high first pass metabolism are not used to incorporate into CDDS?.
Answer:
CDDS by its means releases drugs at a predetermined rate, the slower release may enhance the first pass metabolism of the drug and drug may not be available even in plasma, hence they are not incorporated in CDDS.
E. Enlist uses of mucoadhesive in drug delivery:
Answer:
Mucoadhesive drug delivery systems have a wide range of applications due to their ability to adhere to mucosal surfaces and prolong the residence time of the drug. Here are some key uses:
-
Oral Drug Delivery
-
Buccal and Sublingual Delivery
-
Nasal Delivery
-
Ocular Delivery
-
Vaginal and Rectal Delivery
-
Gastroprotective Systems
-
Wound Healing
-
Targeted Drug Delivery Vaccination
-
Controlled Release