Introduction.
Transdermal drug delivery systems (TDDS), also known as "patches," are dosage forms that are designed to deliver a therapeutically effective amount of drug through the skin of a patient.
TDD is a painless method of systemic drug delivery that involves applying a drug formulation to intact and healthy skin.
The drug penetrates the stratum corneum first, then the deeper epidermis and dermis, with no drug accumulation in the dermal layer.
When a drug enters the dermal layer, it is available for systemic absorption through the dermal microcirculation.
Transdermal delivery outperforms injectables and oral routes by increasing patient compliance and avoiding first pass metabolism.
Transdermal delivery not only provides controlled, consistent drug administration, but also allows continuous input of drugs with short biological half-lives and eliminates pulsed entry into systemic circulation, which frequently causes undesirable side effects.
Advantages of TDDS:

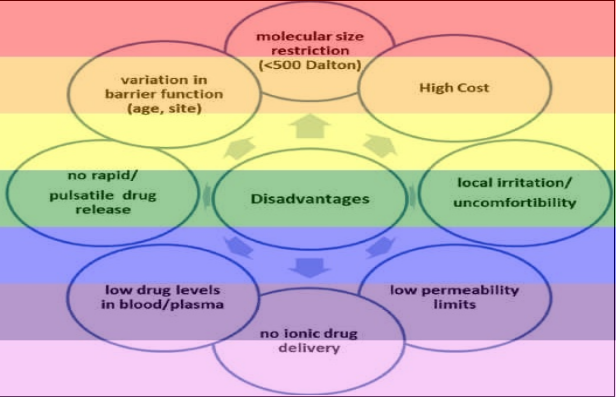
Disadvantages of TDDS:
Anatomy of Skin:
Epidermis:
Stratified, squamous, keratinizing epithelium.
Keratinocytes are the most abundant cellular component (> 90%) and are in charge of the evolution of barrier function.
When keratinocytes migrate to the skin's surface, they change shape, size, and physical properties.
The epidermis is further divided into five anatomical layers, each approximately 100-150 micrometers thick, with the Stratum corneum (SC) forming the epidermis's outermost layer, exposing it to the external environment.
This is the most important layer in transdermal delivery because of its ability to keep water within the body and foreign substances out.
SC is made up of dead cells that have migrated up from the stratum granulosum and are large, flat, polyhedral, plate-like envelopes filled with keratin.
The SC is made up of 10-15 layers of corneocytes that range in thickness from 10-15 m in the dry state to 40 m when hydrated.
Dermis:
The dermis is made up of an extensive microvascular network of structures such as sweat glands, hair follicles, and smaller blood vessels.
To achieve drug delivery through the skin, the drug must first pass through the epidermis and into the dermis, where it can be absorbed by capillaries into the circulatory system.
The inner and larger (90%) skin layer is made up primarily of connective tissue and serves to support the skin's epidermis layer.
The Dermal-Epidermal junction is the boundary between the dermis and epidermis layers, and it serves as a physical barrier for large molecules of drug and cells.
It contains blood and lymphatic vesicles, as well as nerve endings.
Dermis can be divided into two anatomical region;
papillary dermis and
reticular dermis
Papillary dermis is the dermis's thin outermost layer.
Collagen and elastin fibers are mostly vertically oriented and connect with the dermal-epidermal junction in the papillary region.
Hypodermis
The subcutaneous layer, additionally called the hypodermis in histology, is the 3 layers below the dermis.
The subcutaneous layer is an elastic layer that includes a massive range of fat cells that act as a shock absorber for blood vessels and nerve endings.
This layer has an average thickness of four to 9 mm.
The real thickness, however, varies from individual to individual and depends on the body region.
While a molecule enters intact skin, it comes into touch with cell particles, normal flora of microorganisms, sebum, and different substances.
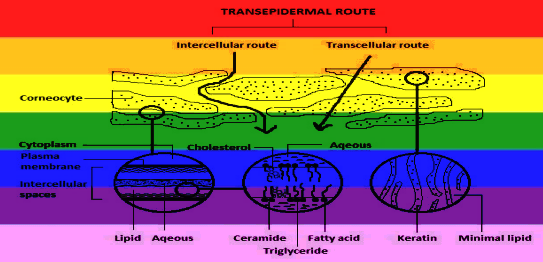
Routes of skin penetration.
Transcellular transport is the primary mode of transport for water-soluble molecules.
It entails the passage of corneocytes through their cytoplasm and the lipid arrangement of the stratum corneum.
The transport pathway for lipid soluble molecules is intercellular; it appears to involve passage through endogenous lipids within the stratum corneum.
The transcellular and intercellular routes are referred to collectively as the trans-epidermal route, as shown below.
Solute molecules may penetrate the skin through the hair follicles, sweat duct or through the sebaceous glands. These passages are collectively known as shunt or appendageal route.
It is generally accepted that the skin appendages comprise approximately 0.1% of fractional area for drug permeation.
Thus, the main focus is to develop permeation strategies through the stratum corneum rather than through the appendages.
The dead cells of the SC, which restrict the inward and outward movement of drug substances and have a high electrical resistance, are the main barriers to absorption.
The SC is a heterogeneous tissue made up of flattened keratinized cells.
These cells' outer layers are less densely packed than the underlying granular layer.
As a result, the lower part of the epidermal barrier becomes more impermeable.
As molecules move from the environment into the skin, the SC serves as the rate limiting barrier, or the tissue that provides the greatest resistance to the movement of molecules.
After applying the dosage form topically, the percutaneous absorption or transdermal permeation can be visualized as a series of steps.
a. Adsorption of a penetrant molecule onto SC surface layers
b. Diffusion through the SC and viable epidermis.
Percutaneous Absorption
It is a three-part process that involves the gradual penetration of substances into different skin layers and their permeation through the skin into systemic circulations:
The entrance of a substance into a specific layer is known as penetration.
Permeation: the transition from one layer to another, which differs from the first layer in terms of both function and structure.
Absorption: the process of a substance entering the bloodstream.
Commonly Asked Questions.
What is a Transdermal Drug delivery system? Write a short note on Anatomy of the human skin.
What is a Transdermal Drug delivery system? Discuss different routes from which drug gets absorbed through the skin.
What is a Transdermal Drug delivery system? Give its advantages and disadvantages.
Write a short note on Stratum corneum and its importance in TDDS.