Formulation Approaches of TDDS.
TDDS can be formulated by different ways as follows,
Polymer membrane permeation controlled TDDS.
Polymer matrix diffusion controlled TDDS.
Adhesive Dispersion – Type Systems.
Microreservoir dissolution controlled TDDS.
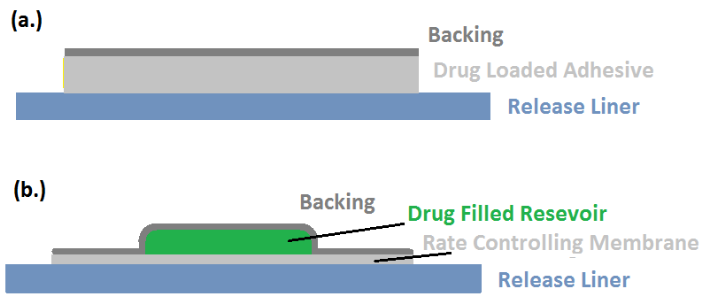
Polymer membrane permeation controlled TDDS:

A polymeric membrane that controls flow rate is positioned between a backing laminate that is drug-impermeable and a drug reservoir.
The drug is evenly distributed throughout the drug reservoir compartment in a solid polymeric matrix (like polyisobutylene) and suspended in a viscous, non-leachable liquid medium (like silicon fluid) to create a paste-like suspension.
A polymeric membrane that controls rate can be either microporous or nonporous, such as ethylene-vinyl acetate copolymer.
Estraderm (used twice weekly to treat postmenopausal syndrome) and Duragesic (used to manage chronic pain for 72 hours) are two examples of this type of patch.
The intrinsic rate of drug release from this type of drug delivery system is defined by
{dq/dt}=Cr/1/Pm+1/Pa.
Where,
Cr = Concentration of drug in the drug reservoir.
Pa= Permeation Coefficient of adhesive layer.
Pm= Permeation Coefficient of rate controlling membrane.
Polymer matrix diffusion controlled TDD system:

This method involves uniformly dispersing drug particles in a hydrophilic (or lipophilic) polymer matrix to create the drug reservoir.
A disc with a specific surface area and controlled thickness is then formed from the resulting polymer matrix.
The medicated disc is then moulded onto an occlusive base plate in a compartment made of a drug impermeable backing.
The film is then covered in adhesive polymer around its perimeter.
Examples include the 0.5g/cm2 daily dose of nitro-glycerine-releasing transdermal therapeutic system for angina pectoris.
Rate of drug release in this system is given by the equation
dq/dt = {ACpDp/2t}1/2
Where,
A= Initial drug loading dose dispersed in polymer matrix
Cp = Solubility of drug in Polymer
Dp = Diffusivity of drug in Polymer since Cp is equal to Cr.
Adhesive Dispersion – Type Systems:
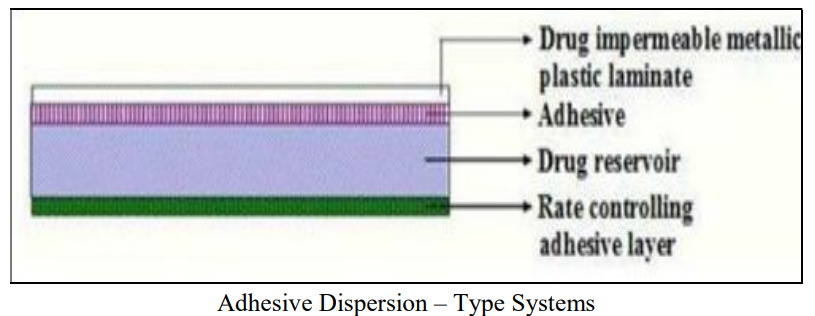
This is a streamlined version of membrane permeation-controlled systems.
In this system, the drug and particular excipients are added directly to the adhesive solution.
The solvent is then removed by drying the thin films that were cast after they were combined and mixed.
The drug reservoir (film) is then sandwiched between the rate-regulating adhesive polymer membrane and the banking laminate.
The rate of drug release from this system is given by,
dq/dt = Cr.Ka/r .Da/ha
Where
Ka/r = Partition co-efficient for interfacial partitioning of drug from reservoir layer to adhesive layer.
ha= Thickness of adhesive layer.
Da= Diffusion Coefficient of a derive layer.
Examples: Isosorbide dinitrate releasing TDDS – 24 hr, Used in Angina Pectoris Verapamil releasing TDDS – 24 hrs, used in Hypertension.
Microreservoir dissolution controlled TDD system:

It's a hybrid system of reservoir and matrix dispersion drug delivery.
The drug reservoir is formed in this system by first suspending the drug solids in an aqueous solution of a water-miscible drug solubilizer, such as polyethylene glycol, and then homogeneously dispersing the drug suspension with a controlled aqueous soluble lipophilic polymer using high shear mechanical force to form thousands of un-leachable microscopic drug reservoir.
Commonly asked questions:
What is TDDS? Discuss various formulation approaches for making a TDDS.
Write a short note on,
Polymer membrane permeation controlled TDDS.
Polymer matrix diffusion controlled TDDS.
Adhesive Dispersion – Type Systems.
Microreservoir dissolution controlled TDDS.
Labels: NDDS