Introduction:
Urine is a waste material formed by Kidneys after filtering the blood, the system involved in formation and excretion of urine is called “Urinary System”.
Like other systems of the body, the Urinary system also works in coordination with other systems.
It plays a vital role in maintaining homeostasis along with the respiratory system and cardiovascular system.
The branch of science that deals with the structure, function, diagnosis and treatment of diseases of Kidneys is called Nephrology.
The study of the Urinary system is covered in Urology.
Urinary System:
It consists of,
Kidneys.
Ureters
Urinary Bladder.
Urethra.

Urethra.
It is a muscular tube that transports urine from the bladder to outside the body for disposal.
It's the only organ of the urinary system that differs in male and female sexes.
It starts from the basal trigonal part of the urinary bladder.
Draining of urine is regulated by two types of sphincters
Internal Urinary Sphincter (Smooth muscle)
External Urinary Sphincter (Skeletal Muscle).
Female Urethra:
It is short and 4cm in length.
Starts from the urinary bladder and opens above vaginal opening, medial to labia minora.
Male Urethra:
It is longer and is about 20cm in length.
It starts from the bladder and opens at the tip of penis.
It has four parts,
Preprostatic Urethra
Prostate Urethra
Membranous Urethra.
Spongy (Penile) Urethra.
Male urethra also serves the functions of reproductive system i.e. carrying the sperms outside the body.
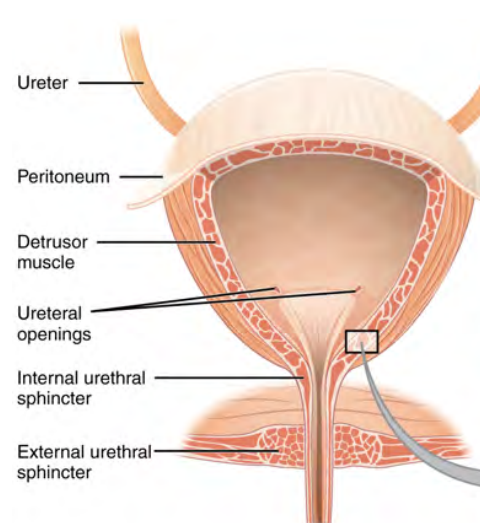
Urinary Bladder.
It is a muscular bag made up of smooth muscle and lies in the “pelvic cavity.”
It is “Pear Shaped” but becomes “Oval” when filled with urine.
It is divided into,
Body
Neck
It has three openings,
Two openings for ureters at body.
One for the urethra in the neck region.
The three openings form a triangle called “Trigone”.
Histology:
Inner Layer: Mucosa (Transitional epithelium).
Middle Layer: Muscular layer (Smooth Muscles).
Outer Layer: Fibrous Layer (Connective Tissue).
It acts as a temporary reservoir for urine.
Internal urethral sphincter from the upper part of urethra controls urine flow.
External urethral sphincter is skeletal and hence voluntary.
Ureters.
Two in number from each kidney.
These are muscular tubes that transport urine from the kidney to the urinary bladder.
25-30 cm long and 3mm in thickness.
They start from the renal pelvis and end in the posterior wall of the urinary bladder.
Histology:
Inner Layer: Mucosa (Transitional epithelium).
Middle Layer: Muscular layer (Smooth Muscles).
Outer Layer: Fibrous Layer (Connective Tissue).
Its function is to transport urine.
Kidneys.
External Anatomy of Kidney:
They are “Two” in number, reddish in color and bean shaped in appearance.
Each lie on either side of the spine, well protected by ribs, muscles and adipose tissues.
Each kidney weighs around 150gm, male kidneys are slightly larger than female kidneys.
They are 10-15 cm in length, 5-7cm in width and 3cm thick.
Near the center of the concave border of the kidney there is a deep vertical fissure called “Renal Hilus” from which blood vessels, lymphatic vessels, nerves enter and exit the kidney, and ureters also come out of the kidney through it.
Coverings of the Kidneys:
Renal fascia: outermost covering. (Dense connective tissue).
Adipose Capsule: Middle covering of adipose tissue that acts as shock absorbant.
Renal Capsule: Inner covering of connective tissue.
On top of each kidney there is a “Suprarenal Gland” also called “Adrenal Gland” which secretes “Aldosterone” and directly affects functioning of the kidney.
Internal Anatomy of Kidney:
A longitudinal section of kidney shows “Two” distinct parts,
Renal Cortex (Outer)
Renal medulla (Inner).
Renal columns are connective tissue extensions that come from renal cortex to renal medulla.
In between renal columns there are characteristic structures of the kidney called “Renal Pyramids” and “Renal papillae”.
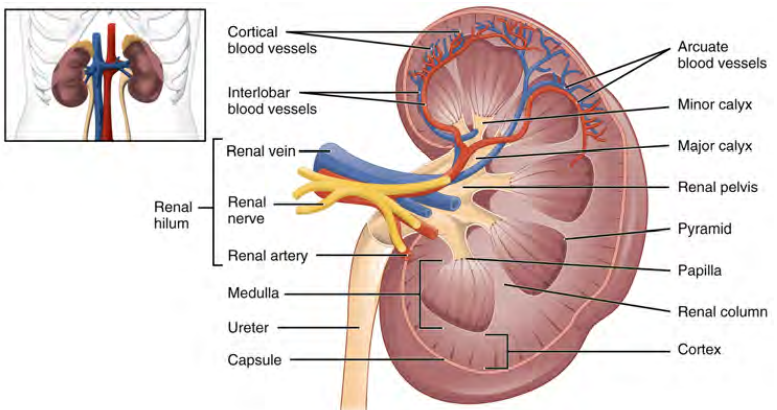
Renal pyramids are conical areas present between two renal columns.
Each human kidney contains around 10-18 renal pyramids.
Renal papilla is the location where urine from collecting ducts is poured in renal calyx.
This is the area where collecting ducts merge with each other to form “papillary Duct”.
Renal calyx is a chamber through which urine from the papillary duct is poured in the renal pelvis.
Renal calyces are of two types,
Major calyx (Receives two or more minor calyces)
Minor calyx.
Renal pelvis is a funnel-like structure formed by merging two to three major calyces, it narrows to form the “Ureter”.
Renal sinus is a cavity in the kidney formed by merging renal pelvis and renal calyces.
Renal hilum is the area of the kidney from which nerves, lymph and blood vessels enter and exit the kidney.
Nephron
Structural and functional unit of kidney.
Each kidney contains around “ One Million” nephrons.
Present in the renal cortex as well as in renal medulla.
Two types:
Cortical Nephrons:
Superficial.
Originate in the cortex and extend for a short distance in medulla.
Constitute around 80-90% of the total nephrons.
Juxtamedullary Nephrons:
Lie deeper.
Originate at the junction of medulla and cortex, go deeper in medulla.
Constitute around 10-20% of the total nephrons.
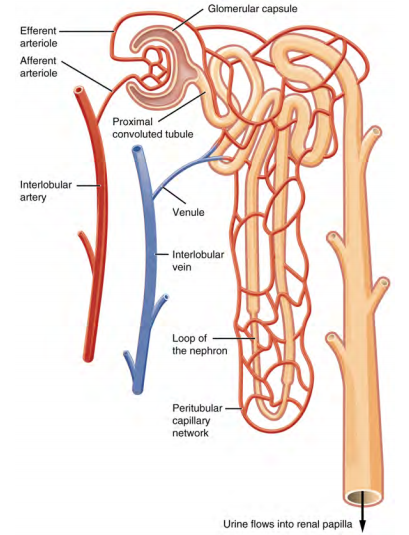
Each nephron consists of two units:
Renal corpuscle. (Filtration Unit) It is made up of,
Glomerulus.
Bowman's Capsule
Renal Tubule. (Transportation Unit) it is made up of,
Proximal Convoluted Tubule (PCT).
Loop of Henle.
Distal Convoluted Tubule. (DCT)
Renal Corpuscle:
It is a filtering chamber where plasma is filtered.
It has two components,
Glomerulus.
Bowman’s Capsule.
Glomerulus is a bunch of capillaries, blood enters in glomerulus via afferent arteriole and exits through efferent arteriole.
Afferent arteriole has a large diameter and efferent arteriole has a smaller diameter, this difference between diameters causes increase in pressure inside glomerulus which facilitates filtration.
Bowman's capsule is a funnel shaped part of nephron surrounding glomerulus.
Bowman's capsule’s outer wall called the parietal layer is separated from the inner wall called the visceral wall by a space called “Capsular Space”.
Bowman's capsule and glomerulus together form a “malpighian body”.
Juxtaglomerular apparatus is a specialized structure of cells that plays an important role in blood pressure maintenance.
“Filtration Membrane” is the contact point between glomerular capillaries and Bowman’s Capsule.
Blood from afferent arteriole enters glomerulus and is filtered i.e. blood cells, protein molecules are retained in capillary while plasma with solutes with smaller size escape from small pores on capillaries to capsular space and then to the renal tubule.
Renal Tubule:
It starts from a bowman's capsule and ends at collecting tubules.
Anatomically it is divided into three parts,
Proximal Convoluted Tubule (PCT).
Loop of Henle.
Ascending Loop of Henle.
Descending Loop of Henle.
Distal Convoluted Tubule (DCT).
Proximal Convoluted Tubule (PCT):
It starts from Bowman’s capsule and continues down the descending loop of Henle.
It has an inner lining of cuboidal epithelium having microvilli brush border (just like epithelial cells in the small intestine), which increases surface area for fluid absorption.
It absorbs ions like Na & Cl, water and glucose.
It absorbs actively hence contain very large number of mitochondrias to produce ATPs
Loop of Henle:
It is divided into two parts,
Descending Loop of Henle. (part going downwards)
Ascending Loop of Henle. (part going upwards)
It is present between PCT and DCT and has sharp hairpin like structure.
It deals with maximum fluid absorption, it is more long in animals present in the desert.
Distal Convoluted Tubule (DCT):
The highly coiled part starts after ascending Loop of Henle.
It contains simple cuboidal epithelium.
It is shorter as compared to PCT.
Collecting Duct:
DCT continues to form collecting ducts.
Collecting ducts are connected to many nephrons.
It contains columnar epithelium.
Physiology of Urine Formation
The main function of the kidney is to clean the plasma, the waste product formed in the process is called “Urine”.
The urine formed in kidneys is transported via ureters to the urinary bladder, the temporary urine storage site, urine is then excreted from the body by a process called “Micturition”.
Urine is formed in kidney in following three steps,
Glomerular Filtration
Selective Reabsorption.
Tubular Secretion
Glomerular Filtration:
First step in process of urine formation.
It occurs in the ‘renal corpuscle’ at the ‘filtration membrane’.
Afferent arteriole has a large diameter and efferent arteriole has a smaller diameter, this difference between diameters causes increase in pressure inside glomerulus which facilitates filtration.
The blood cells, plasma proteins and any other larger molecules normally can not be filtered due to their larger size.
The fluid that passes into the capsular space of the bowman's capsule is called “Filtrate”.
Glomerular Filtration Rate:
The amount of filtrate formed in all renal corpuscles of both the kidneys per minute is called “Glomerular Filtration Rate (GFR)”.
Normal GFR = 125 ml/min (125x60x24. 180 lit. per day)
Selective Reabsorption:
The filtrate after entering in the “renal tubule” gets reabsorbed.
About 99% of the filtrate is reabsorbed and enters the blood, while only 1% filtrate forms the urine.
The movement of water and other solutes from filtrate to peritubular capillaries is called “Selective Reabsorption.”
The term “Selective” is used as only selected substances are reabsorbed e.g. glucose, amino acids, ions like sodium, chloride, potassium, bicarbonate, phosphate etc.
The reabsorption is active as well as passive, involving energy as well as without involving energy.
Selective reabsorption is influenced by various hormones like,
Parathyroid hormones (Thyroid Gland): ↑ reabsorption of calcium and phosphate ions.
AntiDiuretic Hormone, ADH (Pituitary Gland): ↑ reabsorption of water.
Aldosterone (Adrenal Gland): ↑ Sodium and water reabsorption.
Atrial Natriuretic Peptide (Cardiac Atria): ↓ reabsorption of sodium and water from PCT.
Tubular Secretion:
It is the third and last step in urine formation.
In this process various substances are added in filtrate, e.g. Potassium ions, Hydrogen ions, urea, ammonium ions, creatinine certain drugs like Penicillin etc.
Tubular secretion of “Hydrogen Ions” is an important thing in relation to body pH maintenance.

Composition of Urine:
Color: Yellow / Pale yellow.
pH: 6 to 7.5
Volume: 1 to 2 Liters / Day.
Odor: Aromatic, Strong ammoniacal on standing or concentrating.
Composition:
Normal Ingredients:
Water, Urea, Uric Acid, Creatinine, Ammonia, Sodium, Potassium, Chlorides, Sulphates, Phosphates etc.
Abnormal Ingredients:
Glucose: Diabetes mellitus.
Proteins: Kidney infection.
Blood Components: Kidney Infection.
Ketone bodies: Ketosis.
Bile Pigments: Liver disorder, heavy RBC destruction.
Urine production is lowered during sleep and exercise.
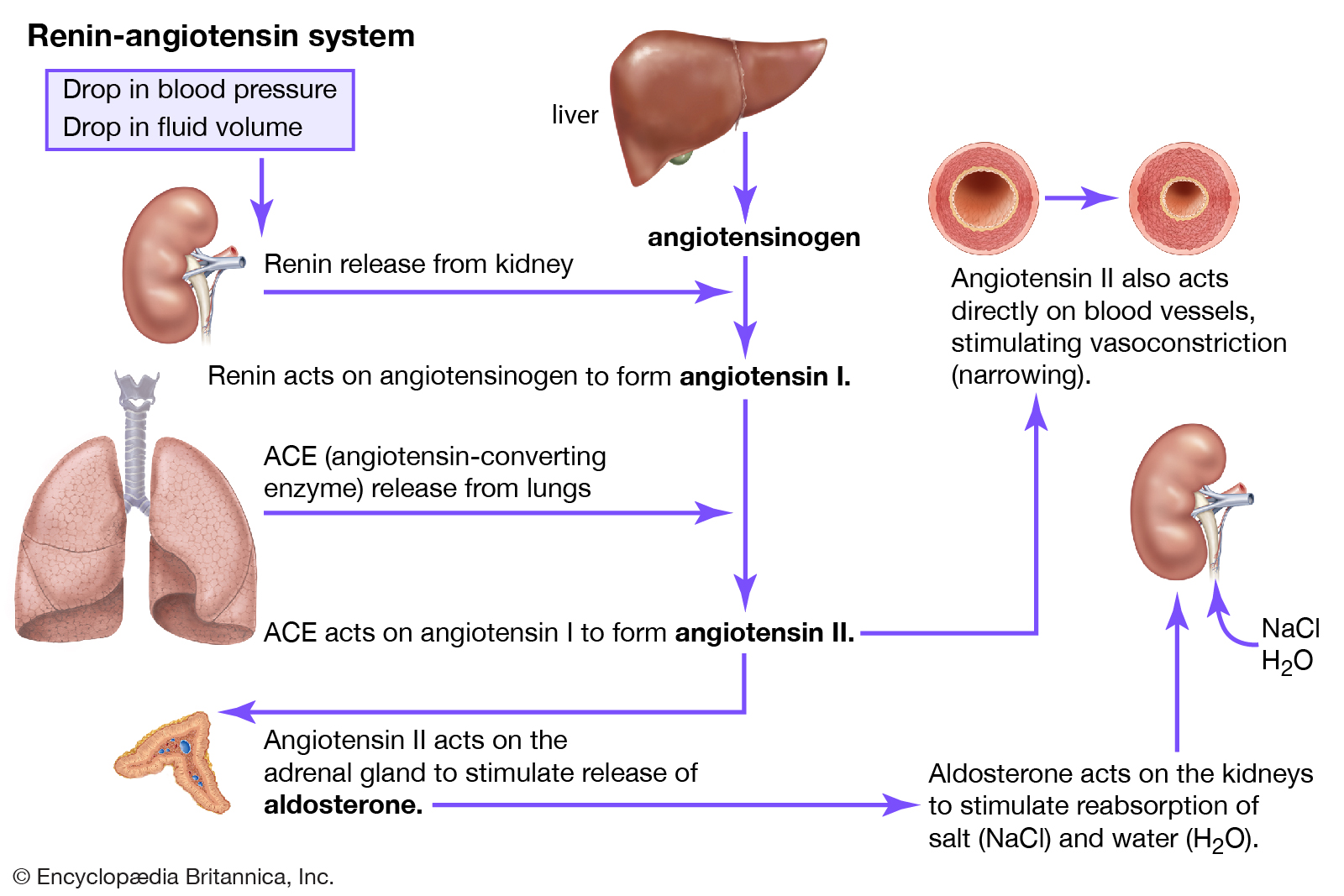
Renin-Angiotensin-Aldosterone System.
Renin-Angiotensin-Aldosterone System is a hormone system that regulates blood pressure by maintaining fluid balance in the body.
Dehydration, Sodium deficiency or hemorrhage are main causes of decreasing circulating plasma levels.
Decreased circulating plasma levels cause low Blood Pressure (low BP).
Decreased circulating plasma levels stimulates “Juxtaglomerular apparatus”.
Juxtaglomerular apparatus secretes a protein called “Renin” in plasma.
Renin activates Angiotensinogen, a plasma protein secreted by liver in plasma to Angiotensin I.
On reaching lungs the Angiotensin I present in plasma get converted to active form Angiotensin II by action of enzyme “Angiotensin Converting Enzyme (ACE)”.
The formed Angiotensin II acts on Angiotensin II receptors present on Adrenal gland and releases “Aldosterone”.
Aldosterone directly acts on kidneys and ↑ Sodium and water reabsorption.
As more water is reabsorbed circulating plasma volume increases causing increased blood pressure.
Angiotensin II also causes vasoconstriction of arterioles causing direct increase in blood pressure.
Role of Kidney in Acid Base Balance of the Body.
Kidneys along with lungs play a major role in acid base balance of the body.
Lungs are very fast but capacity is limited while kidneys are comparatively slower but their capacity is very high.
Lungs maintain acid base balance by converting HCO3 ions to Co2 which is exhaled.
Kidneys largely reabsorb Na+ ions in exchange of H+ ions which are excreted in urine and imparts acidity to urine.
The H+ ions are also excreted in the form of NH4+ and Hydrogen Phosphate Salts.
The H+ ions are formed by help of “Carbonic Anhydrase” enzyme in cells as well as lumen of Renal tubule as,
Micturition Reflex
Micturition is the process by which the urine stored in the urinary bladder is excreted out of the body.
In simple terms “Micturition” is the scientific name of the process of urination.
It is the result of involuntary and voluntary opening of internal and external urethral sphincters.
When the bladder is filled with urine around 150ml there is an urge to urinate, while it can be easily ignored.
When the bladder is filled by urine around 300-400 ml the urge to urinate becomes hard to ignore which results in opening of both the urethral sphincters causing excretion of the urine.
The nerves which play important role are;
Pelvic nerve.
Pudendal nerve
Hypogastric nerve.
The receptors from which actions are initiated are,
B3 receptors (causes relaxation of detrusor muscles in bladder wall)
M3 receptors (causes contraction of detrusor muscles in bladder wall)
Nicotinic receptors (causes contraction of muscles of external urethral sphincter)
The process of micturition involves following steps;
On filling of the urinary bladder, the stretch receptors in the bladder get activated.
Stretch receptors send faster impulses to the sacral micturition center located in the sacral region.
The impulses are then relayed to “Pons' ' in the brain which activates parasympathetic nerves which cause contraction of detrusor muscles through M3 receptors.
Internal urethral sphincter opens involuntarily following contraction of the bladder.
External urethral sphincter is guarded by skeletal muscle which is relaxed by voluntary control causing voiding (urination).

Disorders of Urinary System:
Renal Calculi:
It is a common disorder of the urinary system characterized by severe renal colic pain in the groin region usually associated with urinary urgency, hematuria, perspiration and vomiting sensation due to formation of mineral stones in the kidney or other parts of the urinary system.
Common calculus (Crystals) are;
Calcium oxalate.
Uric Acid.
Calcium Phosphate.
Causes: Precipitation of mineral salts in urine forming crystals.
Highly acidic or alkaline urine.
High calcium intake.
Low water consumption.
Hyperactivity of “Parathyroid Glands”
Treatment:
Diuretics (to increase urine output)
NSAIDs or Opioids (Pain management)
Citrate and magnesium (Salt formation inhibitors)
Tamsulosin (Alpha adrenergic blocker)
Lithotripsy
Surgery.
Urinary Tract Infection:
This term is used to describe the presence of a large number of bacterias in urine or infection of the part or parts of the urinary system.
Common in females. (Due to smaller urethra).
Symptoms:
Burning sensation during micturition.
Fever
Low back pain
Depending on site of infection they are termed as,
Pyelonephritis: Inflammation of Kidney.
Cystitis: Inflammation of Urinary bladder.
Urethritis: Inflammation of Urethra.
Uretritis: Inflammation of Ureter.
Treatment:
Antimicrobial compounds: Sulphonamides.
Antibiotics: Penicillins, fluoroquinolones etc.
Glomerulonephritis:
It is defined as inflammation of glomerulus of the kidneys and is characterized by presence of blood, proteins and lipids in urine.
Symptoms:
Pink or cola-colored urine from red blood cells in urine (hematuria)
Foamy urine due to excess protein (proteinuria)
High blood pressure (hypertension)
Fluid retention (oedema) with swelling evident in your face, hands, feet and abdomen.
Causes:
High blood pressure.
Diabetic nephropathy.
Infections (Viral and Bacterial)
Immunological disorders.
Kidney Failure:
Also called “Renal Failure”, characterized by reduction of glomerular filtration rate.
Two types,
Acute Renal Failure.
Chronic Renal Failure.